The Supplementary Nutrition Programme under ICDS aims to close the nutrition gap among pregnant and breastfeeding mothers as well as children under the age of six. SNP is provided in two ways: Take-Home Rations (THR) and Hot-Cooked Meals at Anganwadi Centres (AWCs). NITI Aayog’s recent report identifies best practices from states across the Take-Home Rations value chain.
Public policy is often fraught with myriad challenges since they do not have any specific set of solutions and are often interlinked. Some public policy challenges continue for several decades, with periodic improvements over the years. Child malnutrition is one such challenge. The first ever National Family Health Survey (NFHS) in 1992-93 found that nearly half of the children are stunted and underweight. It presented a dismal picture of child nutrition in India. Many schemes have been launched over the last few years to tackle the issue of child malnutrition in India. One such major scheme is the Integrated Child Development Scheme (ICDS), which forms the core of child nutrition in India. It also includes the supplemental nutrition programme (SNP), growth monitoring and promotion, nutrition and health education, immunization, health check-ups, and health referrals in addition to pre-school education under its ambit.
The Integrated Child Development Services (ICDS) programme, which falls under the umbrella of food-based safety nets, seamlessly puts together the “first 1000 days” window of crucial importance while addressing malnutrition in young children and pregnant/lactating women through a variety of services such as the distribution of take-home rations (THR), nutrition health education, etc. The Supplementary Nutrition Programme (SNP) under ICDS aims to close the nutrition gap among pregnant and breastfeeding mothers as well as children under the age of six. SNP is provided in two ways: Take-Home Rations (THR) and Hot-Cooked Meals at Anganwadi Centres (AWCs). Take-Home Rations (THR) are provided to children aged 6 to 36 months as well as pregnant and lactating women through the ICDS programme for consumption at home. Through complementary feeding, THR seeks to address the nutrition gap that exists among new-borns and young children.
We look at the report by NITI Aayog and World Food Programme, ‘Take Home Ration- Good Practices- Across the States/ UTs’ in today’s story. This report on best practises aggregates and analyses THR programme developments across several States and Union Territories to create a list of best practises used in the THR value chain’s execution, from formulations to last-mile distribution.
Anganwadis at a glance
As of 30 June 2021, a total of 13,99,697 Anganwadi Centres (AWCs) are established, out of which 13,89,110 centres are operational. This is an improvement from 13,63,021 operational Anganwadi centres in 2017-18. It is crucial that the AWC surroundings and the spaces around it are kept in a clean condition because children, pregnant women, and breastfeeding women frequently visit the facility and have a higher risk of infection during this vulnerable time. The infrastructure of the AWCs varies in size and is often dependent on the amount of available area. However, basic infrastructural facilities like drinking water facility and toilet facility are absent in more than 1.5 lakh AWCs. Almost 25 percent of the AWCs run in rented buildings, making permanent infrastructure provisioning difficult.
On the human resources and manpower front, a total of 13.14 lakh Anganwadi Workers and 11.73 Lakh Anganwadi helpers, along with 4798 Child Development Project Officers (CPDOs), and 33,616 lady supervisors ensure the smooth functioning of the AWCs. However, as evident from an answer of the government in the parliament in July 2021, approximately 1.94 Lakh posts are lying vacant as of March 2021, across all the Anganwadi Service functionaries. This is a slight reduction compared to 2.42 lakh vacancies in 2018, 2.11 lakh in 2019, and 1.92 lakh in 2020. Among the distribution across the states, five states account for around 1.3 lakh vacancies in 2021.
On the financial side, the funds allocated for the states by the Union Government for implementing Supplementary Nutrition Programme grew consistently from 2011-12 till 2020-21, except for a dip in 2015-16. An exponential jump can be seen since 2016-17. This could be due to the setting up of National Nutrition Mission with an outlay of Rs. 9,046 Crores for three years, starting from 2017-18. However, we had earlier noted a decline in the budget allocation for both mid-day meals and ICDS in 2022-23. Also, the amount transferred to states increased despite the fall in the number of beneficiaries under the Supplementary nutrition program. It is found that most of the northeastern states receive higher average funds per beneficiary, while Kerala receives the highest among the large states category.
Take Home Ration – Value chain
The National Nutrition Mission (NNM), also known as the Prime Minister’s overarching Scheme for Holistic Nutrition (POSHAN Abhiyaan), has recently given the supplemental nutrition services offered under the Integrated Child Development Services (ICDS) programme a fresh priority. More than 9 crore beneficiaries who are registered at AWCs receive SNP using two delivery methods: Hot-Cooked Meal (HCM) and Take-Home Ration (THR). The THR programme seeks to supply supplemental food items for use in households to women who are pregnant or nursing, as well as children aged 6 to 36 months. THR programme accounts for a major share in the ICDS budget, with both the State and Union Governments spending approximately Rs. 13,500 cores on it annually.
The THR value chain starts from procurement, followed by the production model, supply chain management, product formulation, Quality control, packaging and labeling, monitoring, and ends with Social and Behaviour Change Communication (SBCC). All these stages are crucial in ensuring the efficiency of service delivery. We shall look into best practices followed by the states in each of these stages as noted in the NITI Aayog’s report. Below are the criteria for the evaluation of best practices.
Best Practices:
Procurement
- Since huge funds are involved in procurement, transparency and quality in procurement become of utmost importance. The THR procured should conform to technical and nutritional standards set by the ministry.
- Three different models of procurement were identified as good practice – procurement through e-tendering in Tamil Nadu and Delhi, procurement based on quality parameters like Telangana, and procurement through Non-profit organizations like Chandigarh are shortlisted.
- In Tamil Nadu, an all-India tendering process is followed, while in Telangana, procurement is done by the State-owned Telangana Oil Federation and Telangana Foods. Additionally, the Superior quality of red gram SPLIT FOTKA SORTEX is only procured. In Chandigarh, 4 non-profit organizations procure 350 AWCs, while the prison department procures another 100 AWCs.
Production Model
States can contract production to either private or government entities. The THR production facilities are managed by local entities like the Women Self-Help Groups (SHGs) in the decentralized production model. A decentralized production model including SHGs stood out as a good practice when analysing the different ways in which the state governments are contracting the production.
Local production of THR by Women SHGs of Kudumbashree Mission in Kerala, production through Women SHGs with fixed time periods for each of the processes in Odisha, and production by Mahila Supplementary Food Production Centres (MSPCs) led by Women Self-help groups in Karnataka are some of the best examples of involving WSHGs in production.
In Odisha, a total of 568 THR-making units run by around 7000 women manage the entire production cycle, covering 72,602 AWCs and benefiting more than 25 Lakh beneficiaries. In Karnataka, around 137 MSPCs are established, each containing 22-25 members from the vulnerable sections of the society.
Supply Chain Management
- It is an important aspect of the entire THR value chain. This process must be made as transparent as possible to ensure that there are open lines of communication and to ensure an uninterrupted supply of goods. A three level-village, district and state nodal offices should work in unison to make the supply chain process smoother and easier.
- Mo-Chhatua Management Information System in Odisha, PuShTI– Poshan Umbrella for Supply Chain through Tech-Innovation in Gujarat, YSR Sampurna Poshana application in Andhra Pradesh, Strengthening Food Commodities Supply Chain Management (FCSCM) – Online First Contact Resolution and Mobile Application in Telangana, and Engaging Sakhi Mandals SHGs in Jharkhand are some of the best practices identified in supply chain management.
Product Formulation
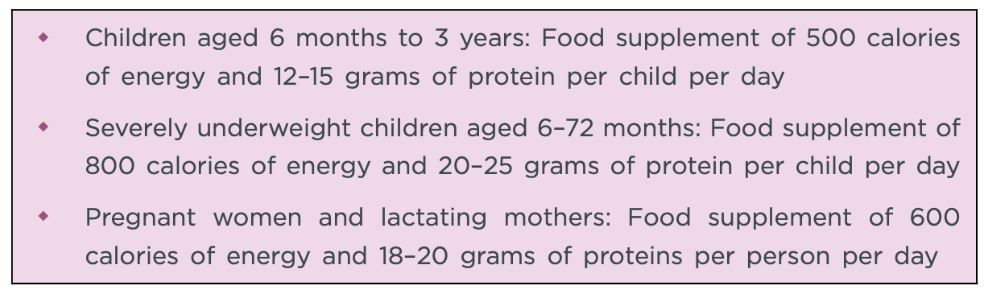
- Since the overall aim is to nourish children, it is important that the THR must be of adequate quality and has good nourishment values. The National Food Security Act, 2013 and the Supplementary Nutrition rules, 2017 have in place calorie and protein norms for THR, that must be followed while providing THR. Below are the Government of India standards, Revised Nutritional and Feeding Norms for Supplementary Nutrition in the ICDS scheme.
- On the fortified THR product formulation, fortified THR with 50% Recommended Dietary Allowance (RDA) in Madhya Pradesh, THR prepared by WSHGs fortified with 11 micronutrients, vitamins and minerals in Kerala, and Premix enriched with essential micronutrients in Gujarat are some of the best practices on fortification of THR.
- On the diversity front, a region-specific diverse menu is important. Himachal Pradesh, Karnataka, Madhya Pradesh, Gujarat, Odisha, and Haryana are examples of region-specific menus. Additionally, the inclusion of millets in THR in Odisha and Chandigarh, eggs and milk in Andhra Pradesh and Haryana, and Ayush THR in Gujarat are some special initiatives.
- For Moderate & Severe Acute Malnourished beneficiaries, increased THR quantity for malnourished children in Chhattisgarh, Rajasthan, Bihar, and Kerala, a Ready-to-Eat Snack prepared by SHGs in West Bengal, and Enriched THR with extra protein, fat and eggs in Telangana and Odisha stand out as best practices in product formulation component.
Quality Assurance/ Quality Control
- Quality control becomes an important aspect of the entire THR value chain. The food supplied through ICDS must be free from toxins, adulterations, and contaminants. It is suggested to adopt the First-in-First-out principle to ensure stocks do not stay for too long and become spoiled.
- Two practices are identified:
- Robust testing mechanism – States like Gujarat, Telangana, Odisha, and Mizoram have this mechanism where the products are inspected for quality through food testing laboratories having national accreditation.
- Batch testing from Government Analytical Labs- Kerala adopted this practice where all samples from each batch are tested for quality.
- On the quality enforcement front, Strict action in case of non-compliance as per prescribed parameters for states like Odisha, Rajasthan, and Mizoram, and Replacement of products in 30 days and penalty charges in Gujarat are some of the good practices in quality management.
Packaging and Labelling
- Good packaging and labelling with all the required information are necessary to ensure that the beneficiaries understand the nutritional messages, and instructions for the usage of THR.
- On the packaging front, Beneficiary specific colour-coded packets in Odisha, Glass bottle distribution in Kerala, and Customized weight-specific packets in Telangana stand to emerge as best practices.
- In the Labelling aspect, Customized messages on packets in Jharkhand, Instructions on preparation methods in Madhya Pradesh and Gujarat, information on ingredients, shelf life, and nutrients in Arunachal Pradesh, and the Informative labelling system in Mizoram stand out as few of the best practices on the labelling.
Monitoring
- Monitoring is essential to ensure accountability in the entire THR value chain. The report identified two kinds of monitoring- Real-time monitoring, and Community participation in monitoring.
- Under Real-time monitoring, GPS enabled monitoring system in Gujarat, and Real-time monitoring using call centres in Jharkhand are good examples.
- Under the community-based monitoring, Community participation in monitoring of THR production and distribution in Odisha, Anganwadi- level Monitoring and Support Committee in Himachal Pradesh, and State level Monitoring Committee in Telangana stand out as best practices in monitoring.
Social and Behaviour change communication
- Any social change is sustainable in the long term only through adequate social and behavioural changes. The link between nutrition and THR is best addressed through social, and behaviour change communication (SBCC) conducted during the process of product distribution. Awareness creation and regular information dissemination are vital in the SBCC strategy.
- On this front, the use of color-coded flyers for improved complementary feeding practices in Kerala, Training of AWW and SHGs on nutrition in Jharkhand, Awareness of nutritional content of traditional and local food in Mizoram, Community based events in Telangana, IEC material focusing on changing behaviour pattern in Odisha, and messaging through digital platforms in Maharashtra emerge as good practices.
- More than 35 lakh programme participants were reached through the ‘Tarang Suposhit Maharashtracha’ platform in Maharashtra. 13 lakh individuals have used the WhatsApp chatbot, sending 50,00,000 messages. On the IVR Helpline, there have been almost 21 lakh calls. To 38 lakh people, broadcast calls and SMS have been sent. Through WhatsApp and the IVR system, more than 76 thousand people have replied to the social audit.
These are some of the best practices in the THR value chain as identified in the NITI Aayog report. It becomes important for the states to cross-learn to adopt the best practices from other states and Union Territories. Sharing new innovative approaches, coupled with regular sensitization of states and UTs on technological adoption in the THR value chain is the way forward.
Featured Image: Supplementary Nutrition Programme

